
ASCO 2024 – Laura’s crossover conundrum

Tagrisso is a knockout on PFS, but only OS will show whether it should be given before patients progress.
Tagrisso is a knockout on PFS, but only OS will show whether it should be given before patients progress.
AstraZeneca’s Tagrisso looks set to put more pressure on Johnson & Johnson’s Rybrevant in EGFR-mutant non-small cell lung cancer, after its Laura trial, in the pre-metastatic inoperable stage III setting, showed an overwhelming progression-free survival benefit versus placebo.
However, the key metric in this broadened setting – relevant given Tagrisso’s cost and added side effects – will be overall survival, especially given that Laura’s design allowed patients progressing on placebo to cross over to Tagrisso. The interim OS data, unveiled today at an ASCO late-breaker, reveal a “positive trend” favouring Tagrisso, but so far are only at 20% maturity.
This will be a major question for regulators to consider. At the time Astra toplined Laura as positive for OS and PFS in April it said it would share the data with global regulatory agencies, but so far there’s been no disclosure about filings or their acceptance.
Maintenance vs Tagrisso on progression?
The issue of OS and crossover is live given Laura’s design.
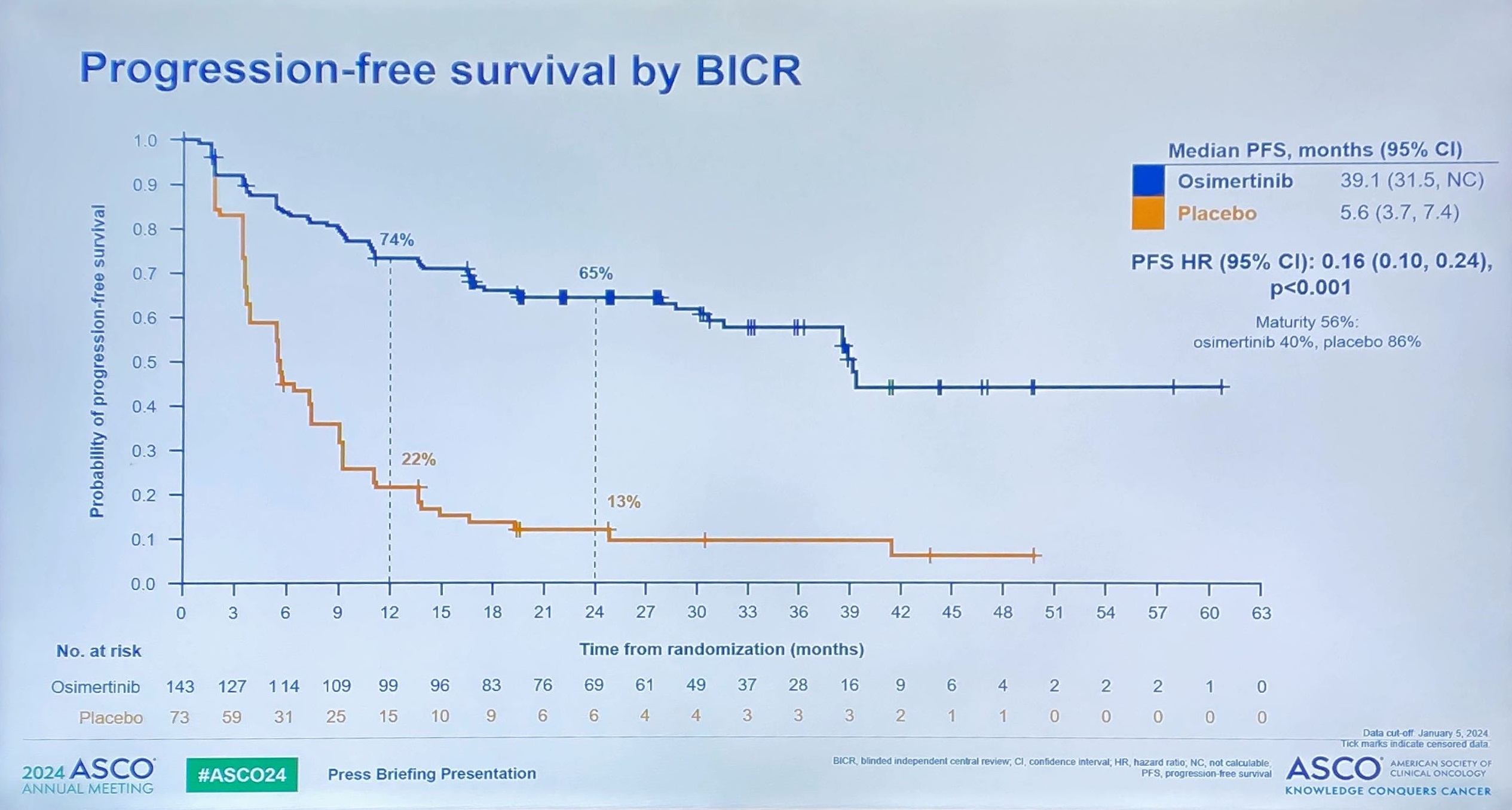
The trial enrolled EGFR-positive, stage III patients who were still in response to chemoradiation, and randomised them to either Tagrisso or placebo. So far the PFS result is an overwhelming hit, with medians of 39.1 months for Tagrisso versus just 5.6 months for control, yielding a statistically significant hazard ratio of 0.16.
So far so good, but 81% of placebo patients who progressed so far have elected to switch to Tagrisso, Dr Suresh Ramalingam of Emory University School of Medicine told an ASCO press briefing.
Because of such a high level of crossover Laura thus starts to resemble a trial comparing not Tagrisso versus placebo, but maintenance Tagrisso versus Tagrisso on progression.
Regulators will need to weigh this carefully; without an OS benefit Tagrisso might have to be reserved until stage III patients progress, for instance.
In comparison, Imfinzi’s approval in the analogous setting of the Pacific study (though in stage III NSCLC patients irrespective of EGFR status) was granted solely on the basis of a PFS benefit versus placebo, though OS data supplemented this later. However, Pacific didn’t allow patient crossover.
All that said, the omens for Laura’s OS analysis are good: Ramalingam said the positive OS trend was evident in the study without making any adjustment for crossover. The next OS analysis will take place at 60% maturity, he added.
A separate consideration is the question of EGFR positivity; EGFR testing is standard in metastatic NSCLC, but not yet in stage III disease. Ramalingam said Tagrisso would become the new standard of care in EGFR-mutant stage III NSCLC, but said the adoption of EGFR testing was crucial to ensure optimal patient outcomes.
1483











