
Warning signs for Xencor

Data on the group’s lead project, the PD-1 x CTLA-4 bispecific vudalimab, are far from emphatic.
Data on the group’s lead project, the PD-1 x CTLA-4 bispecific vudalimab, are far from emphatic.
Xencor’s 16% share price slump this morning might have been partly down to disappointing financials, but lacklustre mid-stage data from its lead in-house asset, the PD-1 x CTLA-4 bispecific vudalimab, will also not have helped.
On the surface, an overall response rate of 33% among metastatic castration-resistant prostate cancer (mCRPC) doesn’t look too bad, especially given the late-line patients involved. But the confirmed response rate was less impressive, PSA data raised questions, and one patient died of autoimmune hepatitis deemed treatment related. Xencor, which yesterday also slipped out news of a 10% headcount reduction, will likely need more to justify pushing on; a go/no-go decision on the project is expected next year.
The data released yesterday after market, during the company’s fourth-quarter earnings, came from Study XmAb717-05, testing vudalimab monotherapy in high-risk mCRPC.
The 14 patients treated so far had received a median of four prior therapies, including chemo, hormonal therapies like Xtandi or Zytiga, and Novartis’s radiopharmaceutical Pluvicto. Among 12 patients evaluable for efficacy four had a partial response, Xencor said, but one of these was unconfirmed.
On this basis, with the usual caveats around cross-trial comparisons and small patient numbers, vudalimab looks a little better than Ambrx’s anti-PSMA ADC ARX517. The latter posted a 22% ORR in a similarly late-line population, which was enough to secure a $2bn takeover by Johnson & Johnson earlier this year.
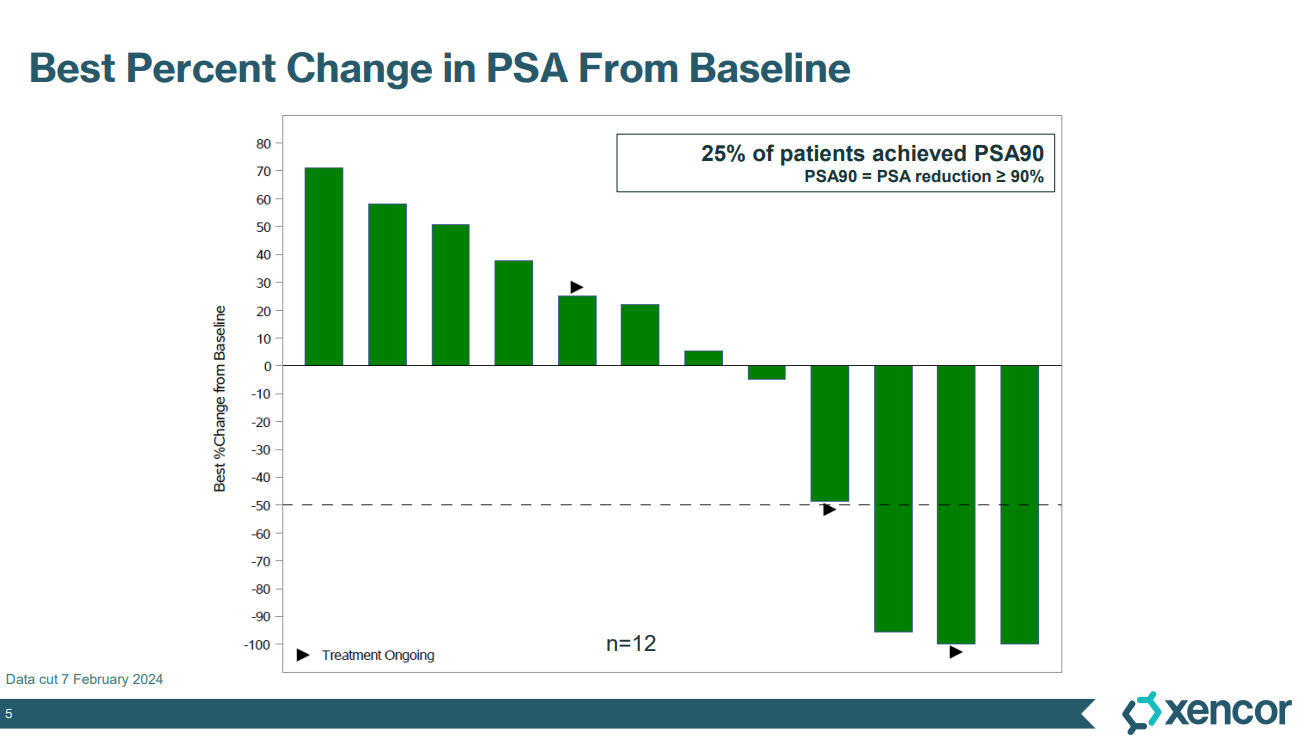
However, vudalimab was arguably less impressive on prostate-specific antigen (PSA) reduction, a widely used prostate cancer biomarker. Yesterday Xencor highlighted the fact that 25% of vudalimab-treated patients achieved a 90% reduction in PSA, an emphatic result. But a closer look shows that these three patients were also the only ones to exceed a 50% PSA reduction; Ambrx previously cited a 52% PSA50 rate with ARX517.
Prostate-specific antigen (PSA) data with vudalimab
And, earlier this week, Janux boasted of a 56% PSA50 rate with its anti-PSMA T-cell engager JANX007; that group hasn’t yet disclosed response rates.
While JANX007 looks relatively safe, Xencor reported a 64% rate of treatment-related grade 3 or greater adverse events with vudalimab. As well as the aforementioned death, there was one case apiece of severe ALT and AST increases.
Xencor previously saw a high rate of treatment-related serious adverse events and discontinuations in its vudalimab/chemo combo prostate cancer trial, Study XmAb717-04. The company modified the chemo dose, but toxicity will be something to keep an eye on when more data emerge next year.
PD-1 x CTLA-4
PD-1 and CTLA-4 blockade is already used in combination, most notably with Bristol Myers Squibb’s Opdivo and Yervoy. However, checkpoint inhibitors haven't fared well in prostate cancer, and Xencor reckons that with vudalimab it can harness a synergistic effect.
Others developing PD-1 x CTLA-4 bispecifics include Akeso, whose cadonilimab is approved in China for second-line cervical cancer and was recently filed there in first-line gastric cancer.
AstraZeneca’s volrustomig is the most prominent bispecific project in the west, but isn't being studied in prostate cancer; instead Astra has phase 3 trials ongoing in lung, head and neck, and cervical cancers, and mesothelioma.
Xencor is also evaluating vudalimab in NSCLC, but here its Study XmAb717-06 has only just begun.
Notable trials of vudalimab
| Trial | Setting | Regimen | Note |
|---|---|---|---|
| Study XmAb717-05 | High-risk mCRPC | Monotherapy | Data Feb 2024, 25% confirmed ORR (3/12); update and go/no-go decision due 2025 |
| Study XmAb717-04 | mCRPC | + chemo | Data at SITC 2022, 14% ORR (1/7), high rate of SAEs; chemo dose modified; update and go/no-go decision due 2025 |
| Study XmAb717-06 | 1L NSCLC | + chemo | Dosing began Q4 2023 |
Source: OncologyPipeline & clinicaltrials.gov.
1464











