
ASCO 2023 – ovarian cancer could provide a role for immuno-oncology at last

Excluding BRCA-positive patients could be the key to Imfinzi’s apparent success in ovarian cancer, Astra’s Duo-O suggests.
Excluding BRCA-positive patients could be the key to Imfinzi’s apparent success in ovarian cancer, Astra’s Duo-O suggests.
Ovarian cancer has so far has proved intractable for anti-PD-(L)1 drugs, but despite this Astrazeneca appears to have teased out a positive result for Imfinzi in this setting. The data, for the Duo-O study of Avastin/Imfinzi/Lynparza, had been toplined positive in April, and have now been presented at an ASCO late-breaker.
This triplet appears therefore to have succeeded where other PD-(L)1/PARP inhibitor combinations failed, possibly because Astra decided to exclude BRCA-positive patients, who would normally be expected to do well on Avastin/Lynparza alone. Nevertheless, questions remain about Imfinzi's contribution, the breadth of the effect, and the robustness of a progression-free survival endpoint.
The validity of PFS in ovarian cancer continues to be the subject of much debate, and there have been cases where a clinical benefit on PFS has later been followed by a clearly negative result in terms of overall survival. This has, for instance, seen use of GSK’s PARP inhibitor, Zejula, narrowed in ovarian cancer maintenance.
Three-arm design
Duo-O had a complex three-arm design, and included two settings. Activecohorts comprised chemo/Avastin/Imfinzi first line followed by Avastin/Imfinzi with or without Lynparza in the maintenance setting; this was compared against a control cohort of chemo/Avastin followed by Avastin maintenance.
Crucially, the trial enrolled BRCA-negative patients only, and its PFS endpoint was split between two co-primaries: an effect in all-comers, and an effect in BRCA-negative patients who were nevertheless positive for some other type of HRD mutation.
The good news is that the Avastin/Imfinzi/Lynparza maintenance triplet met both co-primaries, with p<0.0001. The bad that Avastin/Imfinzi had no advantage over control at all.
The survival curves reveal another nuance. It might have been assumed that HRD-positive patients are driving the all-comers benefit, but in fact in HRD-negatives, some 60% of the Duo-O BRCA-negative population, the triplet also beat control.
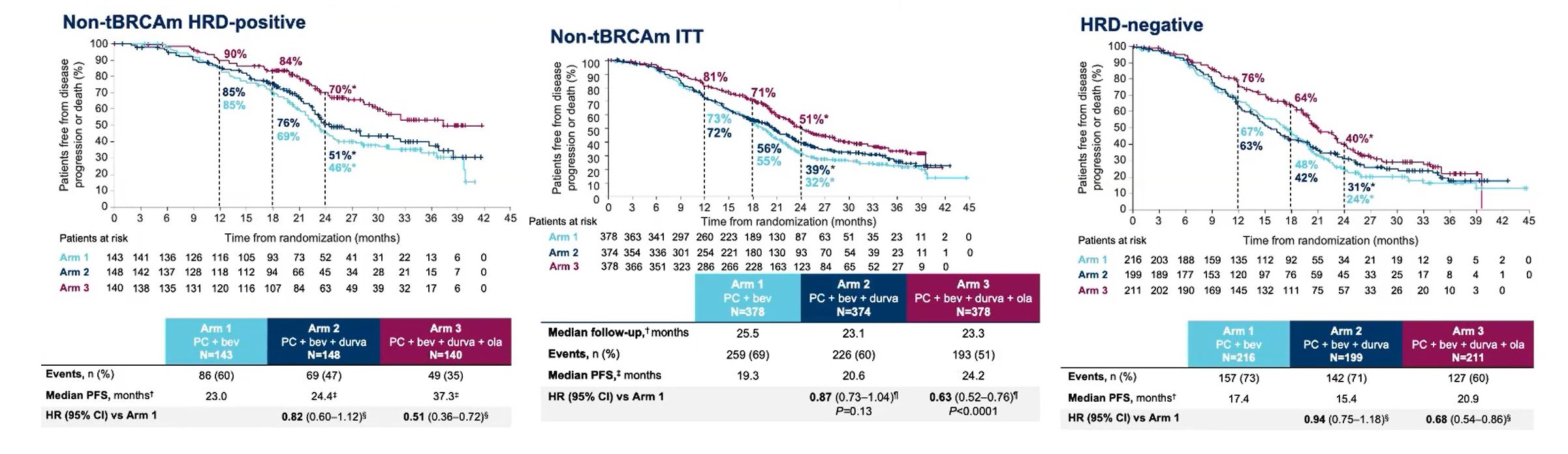
That PARP inhibition should work in patients with no HRD mutation seems counterintuitive. Presenting Duo-O at a pre-Asco press briefing, Memorial Sloan Kettering’s Dr Carol Aghajanian suggested that these patients might not be HRD-negative at all, since the tests on which their HRD status was based “are imperfect”.
Understanding the extent to which HRD-positives are actually responsible for any benefit is key to estimating the possible breadth of any label here. And of course nothing is yet known about OS, a secondary Duo-O endpoint that is still immature.
A separate question is how much benefit Imfinzi is adding; notably only the addition of Lynparza to the maintenance phase brought about a positive result. “If we had to do it again of course we would have a fourth arm that had Avastin and Lynparza maintenance,” said Aghajanian.
Whether Imfinzi is active here goes to the heart of why Duo-O’s positive hit is unexpected. Immunotherapy has tended not to work in ovarian cancer: witness the failures of Roche’s Imagyn-050, Merck KGaA/Pfizer’s Javelin Ovarian 100 and Merck & Co’s Keynote-100 trials.
Next to test the theory will be Merck & Co’s Keylynk-001 trial, which tests Keytruda follows by Lynparza in the maintenance phase, and like Duo-O enrolled only BRCA-negative patients. The Athena-Combo trial of Opdivo and Rubraca was to have read out in the first quarter, but its sponsor, Clovis, has gone out of business.
PD-(L)1 + PARP inhibition in ovarian cancer
| Trial | Setting | Active treatment | Comparator | Note | Brca restriction? |
|---|---|---|---|---|---|
| Roche | |||||
| WO39409* | ≥2L | Tecentriq + Rubraca | Uncontrolled | Ended 2020 after Covid-related protocol amendment, no data reported | None in ovarian cancer cohort |
| Merck KGaA/Pfizer | |||||
| Javelin Ovarian Parp 100 | 1L & maintenance | Chemo + Bavencio, then Bavencio + Talzenna | Chemo +/- Avastin, then Talzenna or Avastin | Discontinued after failure of Javelin Ovarian 100 trial | None evident |
| Merck & Co and/or Astrazeneca | |||||
| Duo-O | 1L & maintenance | Chemo + Avastin + Imfinzi, then Avastin + Imfinzi +/- Lynparza | Chemo + Avastin, then Avastin | Maintenance triplet positive for PFS in HRD+ves, all-comers & HRD-ves | Must be BRCA-ve (including other HRD+ves) |
| Keylynk-001 | 1L & maintenance | Chemo + Keytruda, then Lynparza | Chemo +/- Keytruda, then placebo | PFS in PD-L1+ves & all-comers are co-primaries**; ends Oct 2023 | Must be BRCA-ve |
| Bristol Myers Squibb/Clovis | |||||
| Athena-Combo | 1L maintenance | Opdivo + Rubraca | Opdivo or Rubraca or placebo | PFS primary, data were due Q1 2023*** | None evident |
Note: *not phase 3; **earlier PFS & OS were co-primaries; ***forecast made by Clovis, which later entered bankruptcy and sold Rubraca to Pharma& for $70m. Source: company statements & clinicaltrials.gov.
448











