
ESMO 2024 – Astellas defends its degrader

Despite seeing dose-limiting toxicities, the group is going higher with its KRAS G12D project.
Despite seeing dose-limiting toxicities, the group is going higher with its KRAS G12D project.
ESMO abstract data showed underwhelming results for Astellas’s first-in-class KRAS G12D degrader ASP3082, but the company is pressing on. The group is now dosing higher in the hope that this might lead to more consistent degradation, it told ApexOnco at ESMO.
However, ASP3082 led to dose-limiting toxicities, including liver enzyme elevations, even at some of the lower doses tested. Astellas believes that it can manage these adverse events, but toxicity will be closely watched as it reports more results with this project.
300-600mg, or 800mg?
The ESMO abstract showed an ORR of 8% among 65 evaluable patients in a phase 1 global study in relapsed KRAS G12D-positive solid tumours. Subjects received ASP3082 dosed at 10-600mg once weekly.
During the ESMO presentation, Dr Wungki Park of Memorial Sloan Kettering focused on 48 patients who had received 300-600mg – a dose range that Astellas believes is clinically active.
And within this group Park highlighted 27 patients with pancreatic ductal adenocarcinoma, where there was an overall response rate of 19%. In addition, 23% of 13 NSCLC patients responded – a result Park admitted was very early.
The study also enrolled patients with colorectal cancer, although Astellas’s head of oncology development, Ahsan Arozullah, declined to give response rates here, saying the data were immature.
He described the results so far as “exciting”, but reckons they could improve with a dose of 800mg. “At that higher dose we’re hoping there will be additional and more consistent degradation,” he told ApexOnco.
Toxicity questions
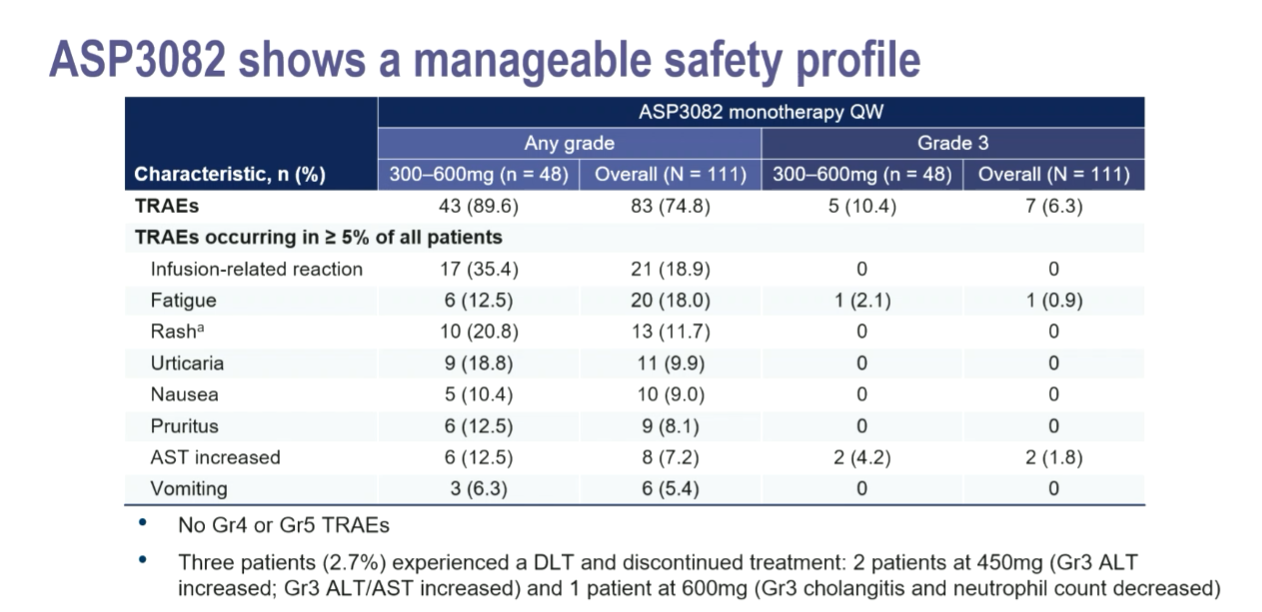
The problem, however, might be toxicity. The trial saw three dose-limiting toxicities, two at 450mg (grade 3 ALT and AST increases) and one at 600mg (cholangitis and a neutrophil count decrease).
Park noted that the liver enzyme elevations didn’t meet the criteria for Hy’s law and, as the protocol didn’t allow for dose reduction, the patients discontinued. Arozullah doesn’t believe that liver enzyme increases are drug related: “In cancer patients you may see a little bit of elevation from time to time.”
Notably, a maximum tolerated ASP3082 dose hasn't been reached, and Astellas says it has the backing of its independent data-monitoring committee to dose higher, he added. “Within our protocol, when we observe a DLT, we actually enrol additional patients at that dose level. To ensure it’s safe, before we go to the higher dose.”
Arozullah even highlighted the “relatively tolerable” safety profile of ASP3082 versus a pan-KRAS inhibitor that he declined to name – likely Revolution Medicines’ RMC-6236. That group recently reported a 20% ORR among 79 PDAC patients, but 87% of patients experienced rash, 6% at grade 3 or above.
The incidence of rash with ASP3082 at 300-600mg, meanwhile, was 21%, and 0% at grade 3 or higher.
This has allowed Astellas to combine ASP3082 with other agents. In PDAC, it’s looking at a chemo combo, and in colorectal it’s already testing ASP3082 alongside Erbitux in the same phase 1 trial. Arozullah wouldn’t say when more data from this study might be available.
5694











